 A Brain Tip of the Frontal Lobes Hat to Andrew for his great article and permission for reprint for my site.
A Brain Tip of the Frontal Lobes Hat to Andrew for his great article and permission for reprint for my site.
Original Article by Andrew T. Austin, UK and his site "Brain, Mind, and Language"
A Brain Tip of the Frontal Lobes Hat to Andrew for his great article and permission for reprint for my site.
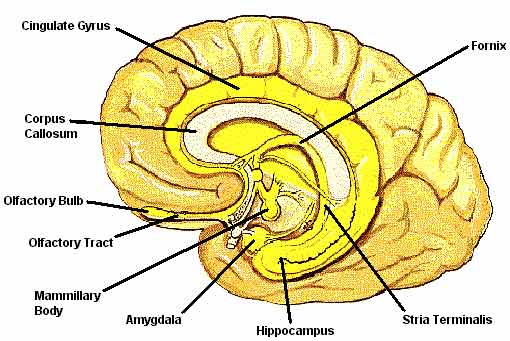 The Amygdala: "A basal part of
the brain, injury to which may cause changes in aggressiveness and
other emotional behaviour." J.Z Young.
The Amygdala: "A basal part of
the brain, injury to which may cause changes in aggressiveness and
other emotional behaviour." J.Z Young.
The amygdala of the brain lies just above the hypothalamus (homeostasis, drinking, sexual reproduction) and provides several functions. Pribram described a girl who had suffered damaged to both amygdalas (although stated in the singular, there is one in each hemisphere) who rapidly became overweight by the compulsion to force food into her mouth, despite denials of hunger. Hunger itself appears to be mediated by the adjacent structure of the hypothalamus, and the function of such is frequently found to be impaired in people with anorexia.
The main difference is that the neurons of the amygdala will respond to the flavors of favored foods, as well as the sights or even cooking sounds of the foods themselves. This effect is important because it had been demonstrated that similar responses will occur in the amygdalas of drug addicts when shown their favourite drug. It is the amygdala that is able to represent the pleasure that is acquired via the foodstuff or drug, and this lends itself when considering the technology of NLP style anchoring - especially with drug users. The cells of the amygdala produce large quantities of endorphins (or as Bandler will call them, "endomorphines") as well as various other hormones, and it is possibly through this effect that the person is able to represent the pleasure of the food or the drug before it has actually been taken. This curious effect is an important consideration for the NLPer, that it is the representation (V, A, K or O/G) itself that can induce the state of anticipatory pleasure in the amygdala.
As well as the above functions, the amygdalas are involved in a wide array of activities ranging from emotions, phobias, traumatic response, rage, anger, aggression, sexuality as well endocrine functions.
The amygdala is a pretty cool bit of kit. Some people even claim to be able to make it 'click' and to control it to release waves of pleasure into the very soul.
 |
One important sex difference exists between male and female amygdalas of many species. Owing to the interplay of the differing sex hormones, males and females will experience pleasure from differing experiences. For example, add a little testosterone and the right setting and the male might quite enjoy having a fight or being simply antagonistic or more commonly play a "boys" video game where the idea is to zoom around and kill everything. Males will enjoy competition and generally throwing each other around. Add a touch of estrogen, and the female will find other things pleasurable. This behaviour, molded by the setting, goes beyond the popular "we are all equal, it's just the environmental conditioning that did it" argument. Counter examples can always be found and are useful in demonstrating other influences upon behaviour. |
One curious effect of an amygdala "adjustment" is that in some occasions aggression will actually increase, at least initially, when the unfortunate creature is given sufficient stimulus (like some prick of a researcher poking the creature with a stick). This effect is soon lost however and appears to be a temporary compensation mechanism of the adjacent structure the hypothalamus (of which there are two - one in each hemisphere).
The amygdala is heavily involved in sex and sexuality with the male amygdala being bit bigger than that of the female The medial part of the female amygdala plays an important role in pregnancy and appropriate coordination of the endocrine system. Stimulation of the amygdala will produce penile erection, sexual sensation (lust), representations/memories of intercourse and orgasm.
One profound effect found to occur in a bunch of monkeys who had their amygdalas destroyed was that whilst they became quite passive and docile, their sex drives shot through the roof. They would quite literally try to screw anything that happened to be convenient in the immediate vicinity. A similar problem affected one poor chap who was arrested whilst attempting to make love to a pavement, who was later found to have amygdala damage. Another effect in the monkeys, similar to the girl mentioned previously, is that they would put virtually anything into their mouths, and would gain weight accordingly. A search of the Fortean Times archives describes several such occurrences of people caught 'in the act' with a variety of inappropriate recipients.
Certainly, whilst working in neurosurgery we would occasionally have a post-operative or brain injured patient who during their 'twilight zone' level of consciousness would masturbate furiously and without relief. As you can imagine this would provide several problems for the patient and for us, not least of all during visiting times. Generally, the patient would not have conscious memory of this once they had recovered.
 Stimulating
the amygdala can also elicit quite profound emotional responses or
rage attacks. The unfortunate Charles
Whitman who spent a tragic 90 minutes shooting anything that moved
from a tower was later found to have a tumour in the region of his
brain of the amygdala, hypothalamus and temporal lobe. This information
was only gleaned after he had been killed, but not before he himself
had killed 14 and gravely wounded another 19 unfortunate people.
Stimulating
the amygdala can also elicit quite profound emotional responses or
rage attacks. The unfortunate Charles
Whitman who spent a tragic 90 minutes shooting anything that moved
from a tower was later found to have a tumour in the region of his
brain of the amygdala, hypothalamus and temporal lobe. This information
was only gleaned after he had been killed, but not before he himself
had killed 14 and gravely wounded another 19 unfortunate people.
Phobic responses are also mediated by the amygdala. Information from
the visual cortex, via the thalamus end up in the amygdala, stimulating
the phobic response. The "fast phobia cure" operates primarily on
the visual system, creating a profound shift in the visual submodalities
(primarily from "associated" to "dissociated" - a significantly "digital"
submodality shift). More on this later.
The amygdala has an interesting function in this respect in the fact that it is the amygdala that processes a wide range of emotional "language". This language involves the 'sounds' of emotion, such as the squeals of delight, the sound that goes with crying, rage, happiness and that high pitched shriek that happens along with a true phobic response.
This provides another consideration when working with a phobia cure, and things might be helped along a bit by maneuvering the client into making a pleasant emotional sound - this will further elicit a positive response from the amygdala along with whatever pleasant anchor the NLPer has triggered.
As a quick aside, the sense of smell which is well known to provoke vivid memories and emotional states, by-passes the thalamus and links to it's own 'relay station', the limbic system. In our research group we experimented with smells as a tool for effective anchoring. Operating through different pathways to those used in the "fast phobia cure", and linking directly into the limbic system we found that favorite childhood smells improved our success rate massively when applied to a 'straight', unstylish fast phobia cure. Curiously, "Matey" bubble bath (other brands are available) and creosote were the most effective/evocative smells from the range we tried. Initially however, in our naivety we had the sequencing wrong and managed to quite successfully anchor the phobia to the smell. This presents a bit of a problem as you can imagine given the interplay of the olfactory bulb and the limbic system.
Another function of the amygdala is it's ability to respond emotional stimuli conveyed through sound, kinaesthetically or by facial expression. It is the amygdala that is able to recognize faces and facial expressions and will respond differently to an angry face as opposed to a happy face. Curiously, it is the left amygdala that responds (activates) to the eye movements of another person and it is the right amygdala that activates when you make eye contact.
Given that EMDR appears to be successful in eliminating phobias and traumatic memory and phobias are mediated primarily in the right amygdala, maybe this begins to give us an insight into how this should be so.
This also gives us a clue as to how we should be presenting ourselves to the phobic/traumatised client when we consider our use of eye contact and our facial expressions.
Often I have encountered NLPers who naively assume that the fast phobia cure/double dissociation will cure anyone of a trauma/phobia/anxiety - some people even go a bit "technique crazy" and go and do a "double dissociation" on anything that moves. It is important to remember that trauma and phobia cure depends on the client having a "reference experience" and not an anticipatory fear.
Le Doux suggests that it is the amygdala that lays down and 'records' unconscious memory, whilst it is the hippocampus that 'records' conscious memory. It appears that genuine post-traumatic stress disorder is mediated by the amygdala. These intrusive memories of unpleasantness tend to become more powerful because they are laid down whilst the person is in a pretty heightened state of awareness with all sorts of stress hormones and neurotransmitters floating about. The effect of these hormones will interfere with hippocampal function and the typical PTSD patient will experience only fragments of the experience ("flashbacks"), but with the full force of the original emotion. The trigger of these flashbacks can be practically anything connected with the original event: an accent, a sound, a picture etc. I have met two elderly PTSD patients who were interned in the Japanese POW camps during WW2, who would freak out at the sound of a Japanese accent. One time whilst working in accident and emergency, a "hospital phobic" patient freaked out only when a cleaner mopped the nearby floor with standard hospital cleaning fluid.
DSM-IV
diagnostic criteria
The diagnostic criteria for PTSD are defined in DSM-IV
as follows:
A. The person experiences a traumatic event in which both of the following were present:
B. The traumatic event is persistently re-experienced in any of the following ways:
C. Persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness (not present before the trauma) as indicated by at least three of:
D. Persistent symptoms of increased arousal (not present before the trauma) as indicated by at least two of the following:
E. The symptoms on Criteria B, C and D last for more than one month.
F. The disturbance causes clinically significant distress or impairment in social, occupational or other important areas of functioning.
LeDoux's mutilations of rat's auditory cortexes demonstrated an interesting feature of some fear responses. Having induced a phobia in the rat (play it a note, give it an electric shock, play it a note, give it an electric shock, etc etc) he smashed out the rats auditory cortex - this should mean that the rat is 'consciously' deaf (a bit like someone having extensive damage to their visual cortex - they are blind, even though their eyes still work perfectly - the thing is, they don't know they are blind owing to the lack of recursion). Whilst the rat could not consciously hear the note that produced the phobia, playing the note still produced an obvious phobic response, because the note still registered in the amygdala and thalamus.
This research helps explain why it can be so difficult to elicit any representation from some people with anxiety/panic attacks and they report, "it just happens," rather than provide information about the stimulus ("How do you know when to have panic?") With conditioned panic it is clearly possible for the stimuli to bypass the conscious regions of the brain and head straight to the areas that produce the fear response. It is possible of course that this effect occurs beneath the conscious threshold and a suitable trance state will enable access to this stimulus.
This effect will mean that the NLPer will need to be rather creative when designing interventions for these clients; the rat subjected to Le Doux's attentions had difficulty distinguishing between the tone he used in the anchoring and other tones would produce a similar phobic response; this response occurs that the unconscious level. It is not unreasonable therefore that the client has no conscious strategy for distinguishing between genuine threatening stimuli and harmless stimuli.
The aim for the NLP Practitioner is to recondition (re-anchor) the response of the amygdala and given what we now know of the amygdala's function, we can begin to design ways of doing this.